You notice it first in the shower drain. Then in your brush. Then, on a bad day, in the mirror, a parting that seems wider than it used to be, or a ponytail that feels noticeably thinner in your hand. Hair thinning in your 30s and 40s is not something that gets talked about enough, and yet it affects more than half of women by the time they reach their mid-forties. It is almost always treatable. But the treatments that work depend entirely on understanding what is causing it, and that part is where most women are left to figure things out alone.
This guide is a comprehensive, evidence-based overview of why hair thins in this decade of life and exactly what the treatment options are in the UK in 2026, from what you can buy at a pharmacy tonight to what a specialist hair clinic can offer.
Why Is Your Hair Thinning? The Real Causes in Your 30s and 40s
Hair thinning in women at this life stage is almost never one single cause. It is usually a combination of factors converging, and identifying all of them is essential to getting the treatment right.
Hormonal shifts, the main driver
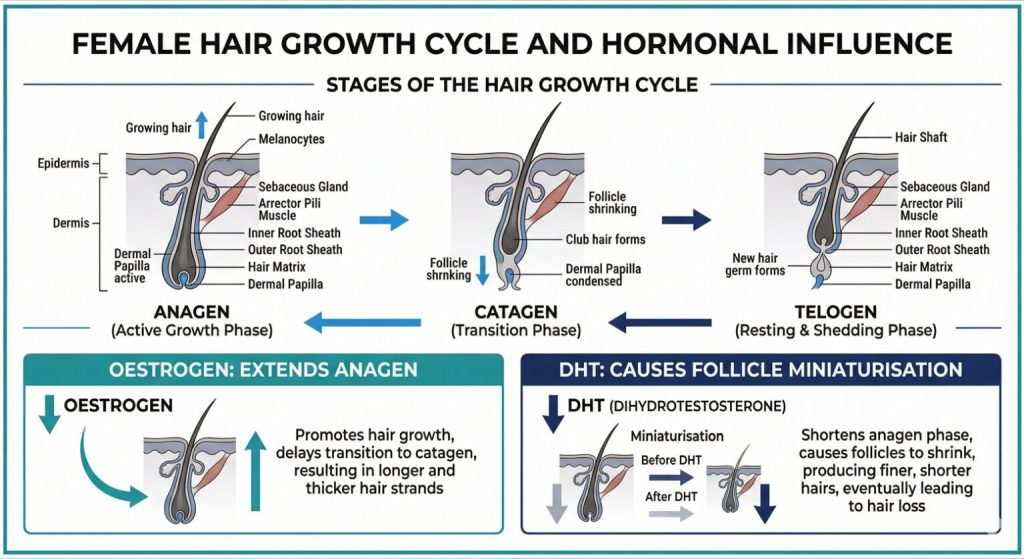
Oestrogen is one of hair’s best friends. It extends the anagen (active growth) phase of the hair cycle and helps maintain follicle health. From the mid-thirties onwards, and especially during perimenopause, which can begin as early as the late 30s, oestrogen levels start to fluctuate. With less oestrogen in play, androgens like DHT (dihydrotestosterone) have a greater relative effect on the follicles. In women with a genetic sensitivity to DHT, follicles gradually miniaturise, producing finer, shorter hair with each cycle. This is female pattern hair loss (FPHL), the most common type of hair thinning in women.
A 2022 survey by Newson Health involving nearly 6,000 women found that 50% reported noticeable hair thinning and 39% experienced hair loss during perimenopause. The average age of perimenopause onset in the UK is 47, but it can begin years earlier.
Nutritional deficiencies
Iron deficiency, particularly low ferritin, is one of the most commonly missed contributors to female hair loss. Studies show nutritional deficiencies are present in 1 in 3 women with perimenopausal hair loss. Vitamin D deficiency, low zinc, and inadequate dietary protein are also well-documented triggers. Unlike FPHL, nutritional hair loss is often reversible once the deficiency is corrected.
Thyroid dysfunction
Both an underactive (hypothyroid) and overactive (hyperthyroid) thyroid can cause diffuse hair shedding across the scalp. Thyroid disorders are more common in women and often emerge in the 30s and 40s. Because the symptoms overlap with hormonal hair thinning, a thyroid test is essential before assuming perimenopause is the only cause.
Telogen effluvium, stress-triggered shedding
This is a temporary but often alarming type of hair loss triggered by a physical or emotional shock to the system, illness, surgery, significant stress, crash dieting, or childbirth. Hair sheds two to four months after the triggering event. The good news: telogen effluvium is usually self-resolving, but it can layer on top of existing hormonal thinning and make the overall situation feel far worse.
Get the Blood Tests First
Before spending money on any treatment, get the right blood tests. This single step is what separates effective treatment from wasted effort. Ask your GP, or a private hair loss specialist, for:
- Ferritin (stored iron), not just haemoglobin; ferritin can be low even when haemoglobin is normal
- Full thyroid panel, TSH, free T3, free T4
- Vitamin D
- Full blood count, B12, folate
- Hormonal profile if PCOS or elevated androgens are suspected, including testosterone and SHBG
These tests can identify treatable causes that, if corrected, can significantly slow or reverse hair thinning without any prescription medication or clinic treatment. If everything comes back normal and the pattern looks like FPHL, then you move to treatment.
Every Treatment Option Available to Women in the UK, Ranked by Stage
| Treatment | What It Does | Best Suited To | Access in UK |
| Topical Minoxidil (5%) | Extends anagen phase; revives dormant follicles | Mild to moderate FPHL; first-line | OTC, pharmacies |
| Oral Minoxidil (low dose) | Systemic approach; stronger than topical | Topical non-responders; diffuse thinning | GP / private prescription |
| Spironolactone | Blocks androgen activity; anti-DHT | Raised androgens; PCOS-related thinning | Private prescription |
| HRT (oestrogen-based) | Restores protective hormonal balance | Perimenopausal / menopausal women | GP or private clinic |
| PRP Scalp Injections | Growth factors reactivate follicles | Moderate thinning; all ages | Private hair clinic |
| Exosome Therapy | 1,000+ growth factors; deeper regeneration | PRP non-responders; advanced thinning | Specialist clinic |
| LLLT (Laser Cap/Device) | Red light stimulates follicle metabolism | All stages; combine with medication | Private / home device |
| Scalp Microneedling | Stimulates blood flow; improves absorption | Adjunct to topical treatments | Clinic or at-home |
FPHL = Female Pattern Hair Loss. OTC = Over the Counter. All prescription treatments require a prescriber consultation. Clinic treatments are private.
Medical Treatments: What Actually Works
Topical Minoxidil, the starting point
Topical minoxidil (Regaine for Women 5% foam) is the only MHRA-licensed treatment specifically for female pattern hair loss in the UK. It is available over the counter. It works by prolonging the anagen phase and reviving dormant follicles. Around 60–70% of women see measurable improvement with consistent use over six to twelve months. The crucial point: you must keep using it. Stopping means the loss resumes within three to six months.
Oral Minoxidil, the stronger alternative
Low-dose oral minoxidil (1.25–2.5 mg daily) has become one of the most significant developments in female hair loss treatment in recent years. A 2025 clinical review found an 80% improvement rate in female pattern hair loss within six months at low doses. It requires a private prescription and blood pressure monitoring, but many women who did not respond adequately to topical minoxidil see notably better results with the oral form.
Spironolactone and HRT
Spironolactone (50–200 mg daily, off-label) is an androgen blocker that addresses the root hormonal driver of FPHL. It has strong evidence in women with elevated androgens or PCOS-related thinning. A clinical trial found that 70% of women on minoxidil plus spironolactone saw improved hair density at four months versus 33% on minoxidil alone.
For women in perimenopause or beyond, HRT (hormone replacement therapy) that includes oestrogen can help restore the protective hormonal environment for hair follicles. Research shows HRT reduces thinning symptoms in approximately 35% of women. It does not treat FPHL directly, but by restoring oestrogen levels it can slow the hormonal contribution to thinning. Decisions about HRT should be made with a GP or menopause specialist who can assess the full clinical picture.
For more on how hormonal changes in perimenopause affect skin and hair, read our guide on menopause skin treatments for the complete picture.
Clinic-Based Treatments: When You Want More
If medical treatments alone are not delivering enough, or if you want to combine approaches, UK hair loss clinics offer several well-evidenced in-clinic options.
PRP (Platelet-Rich Plasma)
A course of three to four scalp PRP sessions, spaced four to six weeks apart, delivers concentrated growth factors directly into the follicle-rich zone of the scalp. It works well alongside minoxidil and is particularly effective for maintaining results after an initial improvement. UK cost: £200–£450 per session.
Exosome Therapy
The newer, more potent alternative to PRP, exosomes contain over 1,000 standardised growth factors versus PRP’s variable platelets. It is the better option for women who have not responded well to PRP or who have more advanced diffuse thinning. UK cost: £400–£1,200 per session. Fewer sessions are needed and results last longer.
LLLT (Low-Level Laser Therapy)
FDA-cleared home laser caps and clinical LLLT devices use red-light wavelengths (620–680 nm) to stimulate mitochondrial activity in follicle cells and prolong the anagen phase. A 2025 systematic review in the Journal of Cosmetic Dermatology confirmed LLLT improves hair density in androgenetic alopecia, with enhanced outcomes when combined with minoxidil. It is a strong, low-risk adjunct for women at any stage of thinning.
Scalp Microneedling
Microneedling the scalp with a dermaroller or professional device creates micro-channels that improve blood flow and significantly enhance the absorption of topical minoxidil. Studies show combining scalp microneedling with minoxidil produces 30–40% better results than minoxidil alone. This is one of the most cost-effective upgrades to a home treatment routine.

How to Build the Right Treatment Plan for You
The most effective approach is layered, no single treatment does everything. Here is a practical framework:
Start here (every woman): Get blood tests. Address any deficiencies. Start topical minoxidil if FPHL is confirmed.
Add this within 3–6 months if topical isn’t enough: Oral minoxidil (private prescription), spironolactone if androgenic profile suggests it, and scalp microneedling to improve minoxidil absorption.
Add clinic treatment if you want to accelerate: PRP every three to six months as a maintenance booster. Exosomes for a more intensive course if PRP isn’t sufficient.
For perimenopausal and menopausal women: Discuss HRT with your GP alongside the above. HRT combined with topical minoxidil is increasingly recognised as the most comprehensive approach for hormonally-driven thinning.
The earlier you act, the more follicles there are to work with. Hair treatments restore and maintain what is there, they cannot revive follicles that have been inactive for years.
Explore more UK health and wellness guides at The Business Brew.
Quick Answers: Hair Thinning in Women
Is hair thinning in your 30s and 40s normal?
Yes, it is common and driven by hormonal changes, nutritional shifts, and genetics. More than 50% of women notice thinning by their mid-forties. It is not inevitable and is almost always treatable if addressed early.
What is the first step if my hair is thinning?
Get blood tests before spending money on any treatment. Low ferritin, thyroid dysfunction, and vitamin D deficiency are common causes that are entirely reversible, and often missed. A GP or private hair specialist can order these.
Does minoxidil work for women?
Yes. Topical minoxidil (5% foam) is the only MHRA-licensed treatment for female pattern hair loss and is effective in 60–70% of women. Oral low-dose minoxidil shows even stronger results in those who don’t respond well to topical use.
Can perimenopause cause hair loss?
Yes. Declining oestrogen during perimenopause reduces its protective effect on hair follicles, allowing androgens like DHT to cause follicle miniaturisation. This can start as early as the late 30s, often before periods become irregular.
Does HRT help with hair thinning?
It can, particularly for perimenopausal women whose thinning is hormonally driven. HRT restores oestrogen’s protective role and reduces the relative androgen influence on follicles. It works best combined with topical minoxidil rather than as a standalone hair treatment.
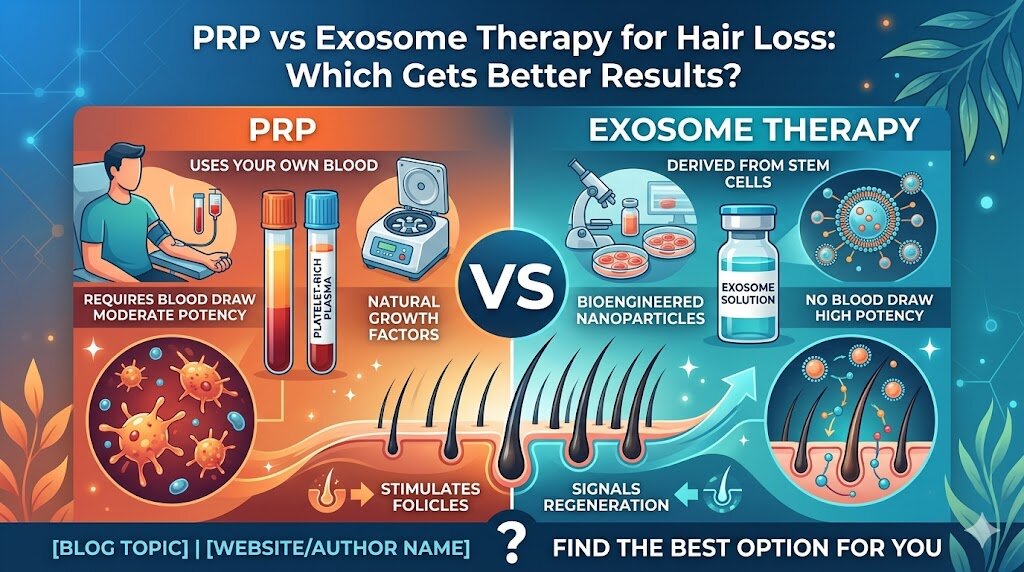
What is the difference between PRP and exosome therapy for hair?
PRP uses your own blood’s platelets to deliver growth factors; exosome therapy uses stem cell-derived vesicles containing 1,000+ growth factors at a standardised concentration. Exosomes are more potent and suited to moderate to advanced thinning or PRP non-responders, but cost more.
How long does it take to see results from hair loss treatment?
Most treatments show initial improvement at three to six months. Minoxidil typically needs six months of consistent use before results are meaningful. PRP and exosome therapy show earlier onset, sometimes four to eight weeks, but full density improvements take three to six months.
Will my hair grow back if I treat it early?
Treating early gives the best chance of maintaining and recovering density. Follicles that are miniaturised but not dead can often be revived with the right combination of treatment. Follicles that have been inactive for many years are harder to restore, which is why acting at first signs matters.
The Bottom Line
Hair thinning in your 30s and 40s is not something you have to accept as an inevitable part of getting older. It is a medical event with identifiable causes and effective treatments. The women who get the best outcomes are the ones who get tested first, start treatment early, and combine approaches rather than relying on a single solution.
Start with the basics, tests, topical minoxidil, and addressing any deficiencies. Build from there. If you need more support, UK hair loss clinics offering PRP, exosome therapy, and specialist prescription protocols can take results significantly further. The earlier you start, the more options you have.